Our Location
The Manor Hospital Beech Rd, Oxford , OX3 7RP

Call Us
07568512719
What is Cataract
- What is Cataract
- Cataract Surgery Technique
- Difficult Cataract Surgery
- Previous Trauma
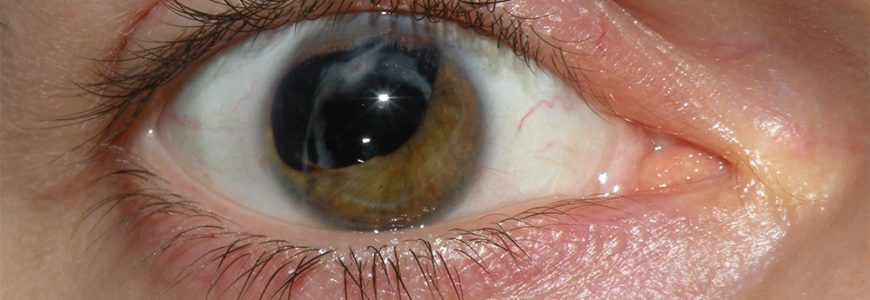
- Hypermature, Dense or White Cataract
- Post Glaucoma Surgery
- Small Eyes in Length
- Angle Closure
The lens can be thought of as a peanut M&M being held by some strings (zonules) in position:
- Outer coloured shell = the capsule
- Chocolate = cortex
- Peanut = nucleus
With time, the lens starts to become cloudy (opaque) and can affect the shell, chocolate or the peanut! The symptoms of the cataract is dependent on which part of the lens starts to become affected:
- Scattering of light causes glare, especially looking at lights (often precluding night driving)
- The lens begins to bend light more strongly, causing a ‘myopic-shift’: distance vision will get worse or more blurred. Paradoxically, this shift can make your vision better if you were long-sighted in the first place!
- Cloudy vision
These symptoms are indications to undertake cataract surgery for vision (or refractive purposes). We have also looked at medical reasons to take out the lens, and indeed other medical indications for surgery exist.
How safe is cataract surgery? The statistics are clear:
- 1 in 1000 people get an infection, that can potentially cause loss of sight in that eye
- 99% of people get better vision
- The posterior part of the capsule separates the cataract from the jelly part of the eye (the vitreous). It is 4 microns thick and can give way in the process of surgery.
- The National Ophthalmic Database describe the capsule giving way or ‘rupturing’ as:
- ‘the most powerful, and only potentially modifiable, predictor of visual harm from surgery.
- The current national benchmark of the posterior capsule (PC) giving way is 2% of all surgeries
- A 2.8mm incision is made in the cornea, this is made in a way which is self-sealing
- The anterior part of the capsule is peeled off (the front part of the outer shell)
- The inner peanut and chocolate (nucleus and cortex) are broken up and sucked out by a hoover type of apparatus (an ultrasound probe)
- This leaves a clear, hollow shell (with only a hole created in the front part of the capsule)
- A new acrylic lens is implanted into this hollow shell and centred
- The wounds are closed, usually without stitches
Occasionally, you will be told that your cataract has greater complexity and should be done by a senior surgeon. Hence your surgery may take longer and have higher risks of complications than standard surgery. This may be due to the inherent nature of your eye or the cataract itself.
Pseudoexfoliation (PXF)
This is a systemic condition typically seen in patient from a Scandinavian origin, although can be present in any ethnicity. In PXF, the body liberates mucoid or ‘dandruff’ type material, which deposits in a host of locations in the body. For instance, it can cause the heart dysrhythmias if it deposits in the cardiac conduction pathway. It is of course its deposition in the eye that interests me the most!
The lens is held in position by strings called zonules and every cataract surgery requires a gentle hand in order to ensure that minimal tension is placed on the zonules. If excessive force is applied, the the zonules can give way or disinsert (‘zonule dialysis’). Hence the outer shell of the M&M is not central cannot accept the implantation of the new acrylic lens. In PXF, the dandruff type material deposits on zonules making them inherently weaker: hence the risk of zonule dialysis is higher. The importance of gentle surgical techniques to preserve the zonules integrity cannot be underestimated. We understand patients with PXF also tend to get severe glaucoma:
- The dandruff type material deposits in the ‘angle’
- Hence, there is impedance to flow of fluid from outside the eye
The chances of encountering difficult surgery with this clinical sign is high: hence it is worth recognising this prior to the date of surgery by assessing the response of the pupil after instilling dilating drops in clinic.
The recognition of PXF pre-operatively can be useful as it enables careful surgical planning:
- Consideration of stabilising the outer shell attached to the zonules by placing a ‘tension ring’
- Doing cataract surgery early, prior to the cataract reaching excessive maturity. The rationale behind this is that less power is required to take out the cataract: hence less stress is imparted on the zonules
- Staged surgeries can be planned
- Rather than implanting the lens in the shell of the M&M, a different lens has to be implanted in a different location. The ones commonly use are:
- Anterior chamber lens (vaulted in the ‘angle’)
- Iris fixed lens
- Quite often, this implantation should be done as a secondary procedure (secondary lens implantation) as it enables the eye to settle ensuring good long term outcomes.
- Rather than implanting the lens in the shell of the M&M, a different lens has to be implanted in a different location. The ones commonly use are:
- The outer M&M shell (capsule) is more difficult to see under the microscope: hence a special stain is used to visualise easier
- The peeling of the anterior part of the capsule is at higher risk of ‘extending’ out to the equator and even to the posterior aspect of the capsule. If that happens, the whole cataract can fall into the posterior part of the eye. This is called a ‘dropped nucleus’ into the vitreous cavity. The extension of the capsule occurs due to the pressure exerted by the sheer density of the cataract itself.
- A greater degree of ultrasound energy is required to suck out the cataract. This causes the posterior capsule to be more labile, with a risk that it can be drawn up into the ultrasound probe and subsequent rupture.
Hence a great deal of caution and care is required operating on these types of cataracts: please see my surgical video of a white cataract
Any surgical procedure in the eye (for example a trabeculectomy) accelerates cataract formation, whereby 90% of patients have a visually significant cataract within two years. The cataract formed is dense, hence the difficulties alluded to above exist.
Furthermore, performing cataract surgery in patients with functioning glaucoma surgery should not be taken lightly. It takes great caution to avoid the glaucoma surgery to avoid failure long term.
If you measured the length of the eye from the front of the cornea to the back, towards the optic nerve, the average length is 24mm. In the narrow angle population, this axial length is much smaller: to the extreme it can be less than 19mm (called nanophthalmic eye).
If the eye is smaller in length, all structures are more crowded, including the ‘angle’. Not only does this predispose to chronic narrow angle glaucoma or acute angle closure glaucoma (link to section on clear lens extraction), it also makes cataract surgery more challenging:
- The peeling of the anterior part of the capsule is at higher risk of ‘extending’ out to the equator and even to the posterior aspect of the capsule. This increases the risk of a dropped nucleus.
- There is less space to safely place the ultrasound probe inside the eye to suck out the cataract. This increases the risk of corneal damage, risking the clear cornea becoming cloudy or opaque. Potentially, this may require further surgical intervention to manage (full or partial thickness corneal grafts)
There are many different techniques in breaking up the cataract before sucking it out. For this difficult cases, I use a ‘chop’ technique which minimises energy utilised and manipulation of the cataract.
If the angle completely closes, the pressure can increase to dangerous levels. This may necessitate emergency cataract surgery to open the angle and establish pressure control. The difficulties encountered in this type of operation:
- Lack of space within the eye, with all the risks alluded to above
- An inflamed eye
- The pupil is often ‘stuck down’, causing increased difficulty in reaching the cataract. Hence the pupil must be ‘stretched’ using various devices, including ‘iris hooks’
It can be seen that to generalise cataract surgery is a mistake: it definitely varies from one person to another. As surgeons, we stratify each operation to calculate the varying risks for each individual. We occasionally recommend variations to our standard practice if the operation demands it. For instance, to increase safety and long term success, if a patient has a small eye and limited space We often opt for the operation to be undertaken:
- Under general anaesthesia
- With the use of a water tablet (a diuretic called mannitol) to seep out water from the vitreous cavity, thus increasing the space within the eye for safe surgery
Refractive Options in Cataract Surgery
Cataract surgery is one of the most frequent, and often most rewarding surgeries performed by Ophthalmologists. It involves: